Lessons Learned From the TEAM Study
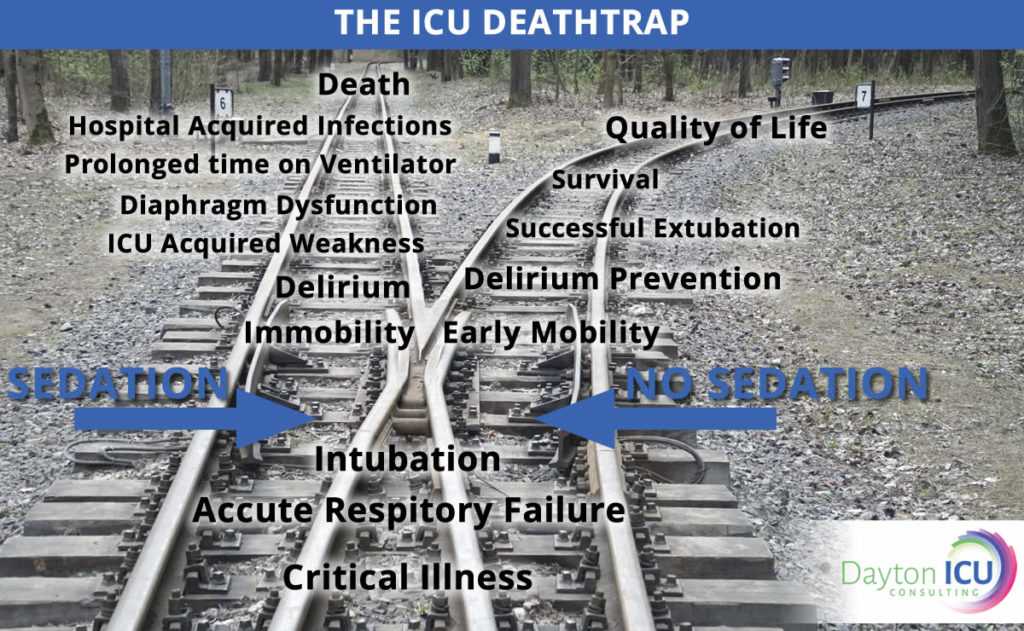
“See? From this we see that mobility does nothing!” This is the common rebuttal that I have received from at least a few physicians in every single ICU I have trained since the TEAM Study was published in The New England Journal of Medicine in 2022. There is often a sparkle of mischief in their