
After working in 11 ICUs and training 14 others, I have seen multidisciplinary rounds conducted in many different ways.
And I’ve also witnessed how easy it is to check the boxes but still miss the mark.
Even in teams that are more progressive with the ABCDEF Bundle who “check the boxes” during ICU rounds, the bundle is often approached something like this at best:
“This is a 75-year-old male patient with a history of hypertension and type II diabetes admitted for acute respiratory failure secondary to influenza A. He was intubated four days ago.”
Intensivist: “SAT?”
Nurse: “He failed his SAT and SBT this morning and sedation is back at X.”
Intensivist: “Ok, we’ll try again tomorrow.”
Charge Nurse/Clinical Nurse Specialist: “What is his CAM and RASS?”
Nurse: “RASS is -1 and CAM is positive.”
At this point, everyone shrugs in apathy as if to say, “Yup, he’s confused. So is the rest of the unit. Welcome to the ICU.”
Charge Nurse/Clinical Nurse Specialist: “Mobility?”
Intensivist: “Yeah… we can order PT and OT.”
Meanwhile, the patient is actually at a RASS of -3 or lower and trapped in delirium believing their organs are being harvested.
He tried desperately to say, “Please don’t kill me!” during the awakening trial but sedation was resumed and he was shoved back into the horrors of delirium.
PT and OT receive the consultation order, but their full schedule does not allow them to see the patient until the next day.
The next morning, they review the chart and see a RASS of -1 documented. When they approach the patient, they find they’re actually at a RASS of -4 and unable to participate in therapy.
What’s more, the conversation during rounds is nearly identical to what was discussed the day before.
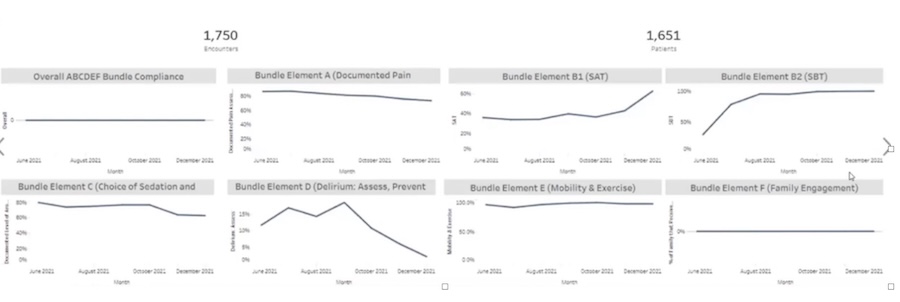
The ABCDEF Bundle boxes are checked and the ABCDEF Bundle dashboard looks compliant, while patients continue to rapidly lose brain function, muscle mass, chances of survival and/or future quality of life.
Then the patient continues to get weaker and more confused, leading to days, weeks, and even months longer on the ventilator.
The unit may have “Centers of Excellence” and/or “Beacon of Excellence” plaques on the wall, but patients continue to suffer preventable harm and mortality.
Moreover, the extra workload and cost of superficially “checking the boxes” without providing the care is unfathomable and unsustainable in this staffing crisis.
In such a culture and process of care, this patient who walked into the hospital with pneumonia will be wheeled into a nursing home with an acute or even chronic brain injury and neuromuscular condition from ICU sedation and immobility.
What could have been a few days of mechanical ventilation can easily turn into days or even weeks of ICU care which turns into an incredible burden on acute care staff as they wait for a nursing home room to open up and battle high risks of readmission to the ICU from aspiration, falls, etc.
ICU Rounds in Awake and Walking ICUs
For teams that truly understand the ABCDEF Bundle as a box of tools to keep patients as awake, communicative, autonomous, and mobile as possible, ICU rounds are entirely different.
These kinds of teams focus on providing care that’s catered towards returning the patient to their baseline function and quality of life. They treat fellow humans, not just diagnose.
And these kinds of teams know that:
1) The ABCDEF Bundle is not just about ventilator liberation but about life preservation.
2) Sedation is not an assumed necessity but a high-risk and abnormal intervention that warrants an indication, explanation, and discussion.
3) Mobility must be a prompt and standard life-saving intervention like DVT prophylaxis.
4) Delirium is a life-threatening organ failure that must be prevented and urgently treated.
5) The ABCDEF Bundle is an essential set of protocols that are just as important as deciding which antibiotic or fluid to give.
This leads multidisciplinary rounds to run much differently and for discussions to go more like this:
“This is a _____ year old M/F _____ (one personal detail that reflects who the patient is as a person and one personal detail that reflects their baseline cognitive and physical function) with a history of _________ admitted for _______.”
And if they’re intubated, these are the kinds of questions that will be asked:
- What is their current RASS?
- How does the patient communicate?
- Have they been educated on delirium?
- What do they report their pain level as?
- If sedation is running, what is the indication for sedation?
- What is the patient’s RASS and status (ICP, BP, Sp02, etc.) when sedation is turned off?
- If their RASS is >0, what is causing this distress and have we treated the cause? Is family at the bedside?
- What is the plan to treat the cause of failure?
- Have we done an SBT today? How did it go?
- Does the patient have delirium?
- If the SBT failed, why did it fail?
If they did fail their SBT, these are the kinds of follow-up questions they’d ask:
- What could be causing this?
- What is the plan to treat delirium?
- What is the plan for follow-up care?
- Have we taught the family about delirium?
- How much sleep did they get last night?
If they report that they got poor sleep, then they’ll be asking things like:
- What is the plan to improve sleep tonight?
- What is their baseline level of mobility?
- Is there a contraindication to mobility? If yes, what is it?
- If the patient is an HLM 1-4, are they appropriate for verticalization therapy?
- What level of mobility did they perform yesterday (tolerance, support needed, duration, etc.)?
- Which member(s) of the family are involved and what support do they need?
- What is the plan for mobility this shift?
Case Study
Now, let’s apply the ABCDEF Bundle and compare this with the first scenario.
“Roger is a 75-year-old male retired welder who loves to build birdhouses. He has a history of type II diabetes and hypertension. He was admitted for acute respiratory failure secondary to influenza A and intubated four days ago.”
Intensivist: “ABCDEF Bundle?
A) Nurse: “Roger uses a clipboard for communication and reports his pain at two out of 10.
B/C) “He failed his SBT this morning because of low tidal volumes and tachypnea from diaphragm weakness which we’re treating with mobility. We’re keeping him on pressure support and keep trying to wean down the support. His RASS is +1 probably because of his hyperactive delirium. He does not have sedation running nor has an indication for sedation.”
D) “For his delirium, his wife is at the bedside and helping him Zoom call his grandchildren. He got four hours of sleep last night and we’re going to try to get him outside today, have him up in the chair, mobilize him twice during day shift, no naps in the afternoon, and night shift will mobilize him one more time, so he should sleep much better.”
E) “At baseline, he was independent and could walk up and down the stairs in his house. Yesterday, he walked 250 feet twice with a walker and took one break. Today we’re going to see if he can go without a break and get him walking that lap twice during day shift and then once on night shift.”
F) “We’re seeing if his son can come stay with him at night to help with his delirium and give his wife a break. They’re helping keep him engaged and we’re leaving restraints off while they’re in the room as they know to keep his hands busy and away from his lines and tubes.”

Conclusion
This patient in an Awake and Walking ICU has high chances of emerging from delirium very soon and being extubated that evening or the next morning.
He has the best chance possible of walking out of the ICU and discharging home from the hospital to resume his normal life after a few days in the ICU.
This is the difference between only “checking the boxes” versus actually providing the care.
Strategic ICU rounds help guide teams to transform care from treating diagnoses to treating people and giving them back lives that are worth living.
Let’s check the boxes on paper and hit a bullseye in practice.
If this resonates with what you’re seeing in your ICU, I can help.
Book a free consultation today and let’s walk through your current approach to mobility and positioning to identify where small shifts could meaningfully improve patient recovery.



