
Throughout my journey in this ICU revolution, I have come to learn that the simplest concepts can be the most profound and the most important.
This is going to sound too basic to be significant but hear me out.
Gravity needs to be considered a standard “medication” in the ICU.
Gravity is the grounding force of life. For most of us, it is all we have ever known during our mortal existence. Its continual presence in our lives doesn’t require conscious awareness or focus.
So, why am I writing an article about gravity as if it’s “news” when it is as old as the Earth?
Aside from space travel, hospitals are one of the only environments in which human bodies are deprived of gravity.


Ironically, gravity is essential to human survival and the overall well-being of the human body.
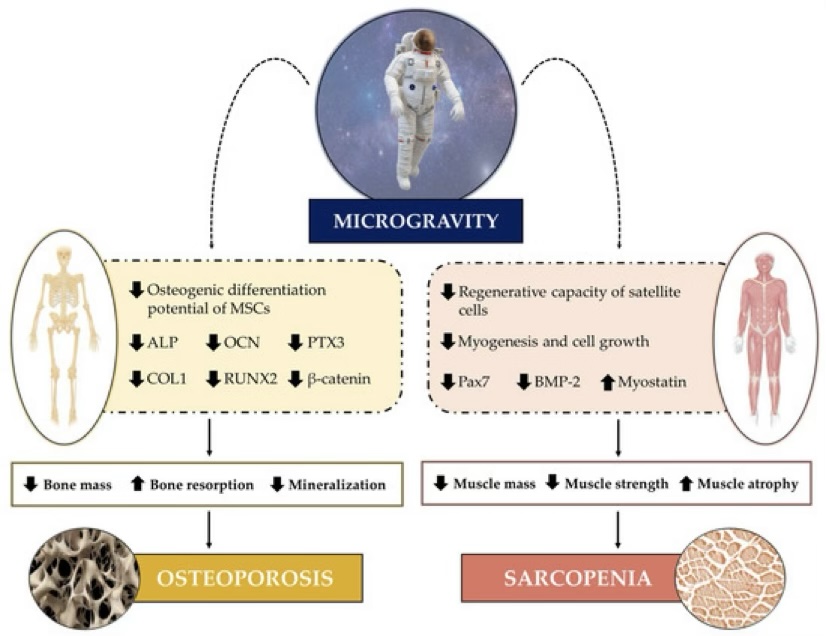
This was not fully appreciated until prolonged space travel was attempted in the ‘60s and ‘70s, when it was quickly realized that these healthy, robust, and athletic astronauts returned to Earth with severe physical impairments such as:
- Muscle loss
- Bone density loss
- Insulin resistance
- Vision impairments
- Vestibular dysfunction
- Orthostatic hypotension
- Immunological impairments
- Cardiovascular deconditioning

In the 1980s, the mechanism responsible for the impact of antigravity was discovered by researcher Joan Vernikos.
And how did she simulate a microgravity environment here on Earth?
She used BEDREST.

Using young, healthy, and strong participants, researchers applied prolonged bedrest and found the same detrimental physical impacts as space travel.
One study involved healthy 23-year-old men on bedrest for one week.
They were eating normally, moving in bed, and not sick. They just could not get up and expose their bodies to gravity.
On average, they lost 1.4 kg of lean muscle and experienced a 5% increase in insulin resistance after just one week of bedrest!
After vast research, we know that depriving the body of gravity impacts the:
Cardiovascular System

Immune System
Musculoskeletal System
Nervous System

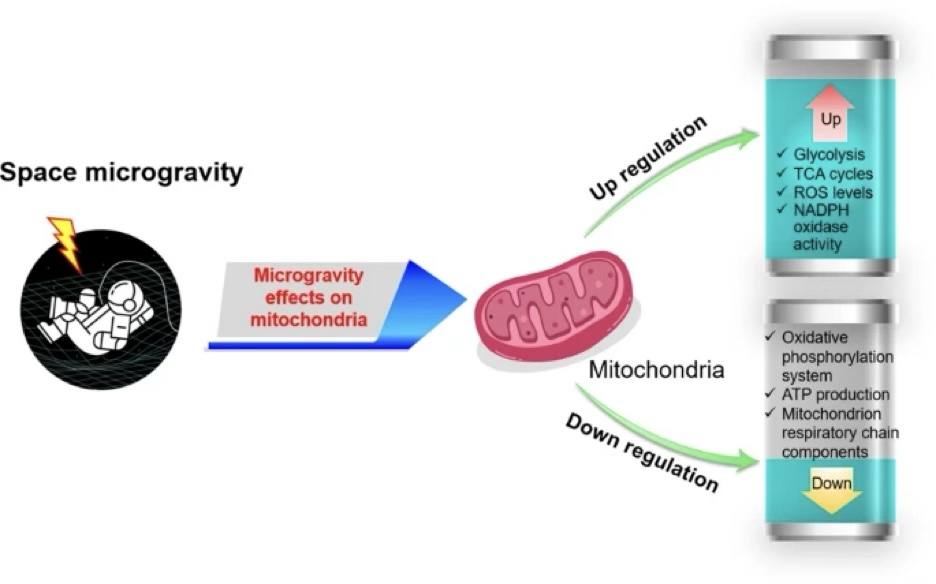
Mitochondrial System
When patients are critically ill, all of these organ systems are already being altered.
And the muscular system alone is being aggressively attacked through numerous pathways.
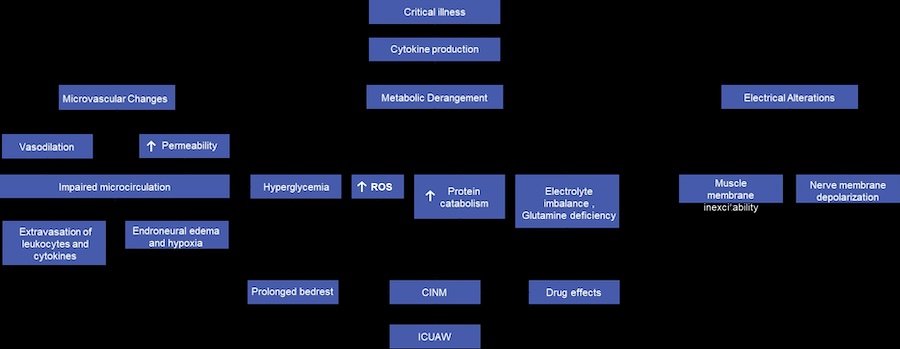
Yet, when our frail and complex patients are critically ill, the standard is to then subject them to prolonged bedrest.

This begs the question: If healthy study participants can rapidly waste away in bed, how much more dangerous is the bed for acute and critically ill patients?
Why then have we built an entire culture and environment of “patient safety” around the bed?
What if we woke up and saw a hospital bed as a high risk and dangerous intervention that should be minimized?

What if we focused our equipment, workflow, and interventions around ensuring early and frequent doses of gravity in the ICU?
How much better could our patients be in and after the hospital?
This foundational knowledge can help clinicians prioritize mobility early on in a hospital admission.
What’s more, it makes them more likely to select mobility interventions that would administer gravity to their patients such as sitting, standing, and walking, rather than in-bed activities.

Hospitals would also be more likely to adapt innovations like combilizers and verticalization beds that can give more complex patients access to gravity in the ICU with more safety and feasibility, along with greater dose and frequency.
Here are a few examples of these kinds of devices:
The Sara Combilizer

The Kreg Catalyst

The Vitalgo Total Lift

All things considered, with the knowledge and tools we have in 2025, gravity in the ICU should be administered promptly to almost all patients early on and throughout critical illness.
Want to learn how to implement and advocate for an Awake and Walking ICU approach?
Contact me for more information or join our monthly meetings for ICU Revolutionists to gain support from fellow clinicians from around the world.


 When patients are so ill that they require a ventilator in the ICU, the antiquated approach of heavy sedation and immobilization should be avoided in order to help prevent the immense burden of physical and cognitive disabilities suffered during survival. To understand this better, listen to Walking Home From The ICU. You will see what ICU consultant Kali Dayton provides to your team.
When patients are so ill that they require a ventilator in the ICU, the antiquated approach of heavy sedation and immobilization should be avoided in order to help prevent the immense burden of physical and cognitive disabilities suffered during survival. To understand this better, listen to Walking Home From The ICU. You will see what ICU consultant Kali Dayton provides to your team.
